Claim: “Providing Funding for Mental Disorders Increases Malingering Rates”
Accuracy Assessment: Largely True
The core claim is Largely True. There is robust causal and observational evidence that financial incentives linked to ADHD and autism diagnoses — through disability benefits (DLA/PIP), school funding mechanisms (EHCP top-up funding), and educational accommodations — do measurably inflate reported diagnosis rates beyond genuine prevalence. A landmark peer-reviewed economic study (Morrill, 2018, Journal of Policy Analysis and Management) found that children in US states with school-level financial incentives for ADHD identification were 15% more likely to report having ADHD and 22% more likely to be on ADHD medication, with causal identification through policy-change variation. In the UK, children’s disability benefit spending has more than doubled in a decade — from £1.9 billion (2013-14) to £4.0 billion (2023-24) — driven almost entirely by awards for learning difficulties, behavioural disorders, and ADHD. The Institute for Fiscal Studies (IFS) explicitly lists “financial incentives to seek EHCPs” as one of the reasons behind the rocketing number of children with statutory SEND provision. A 2021 systematic scoping review published in JAMA Network Open (334 studies) found “convincing evidence that ADHD is overdiagnosed in children and adolescents”, and the BBC has documented — via UK headteachers — cases of parents exaggerating or fabricating children’s symptoms to secure diagnosis-linked benefits. The UK government launched an independent review in December 2025 specifically citing concern that rising diagnosis rates are inflating welfare spending.
The detection of malingering in ADHD assessments is documented as imperfect: the best dedicated screener (SAMS) has a specificity of only 80.1%, meaning approximately 1 in 5 genuine patients could be flagged. Parental proxy reporting — where a parent describes a child’s symptoms — is structurally harder to validate than self-report; there is no direct behavioural observation of the child’s behaviour at home. This architectural weakness in the assessment process is well recognised by clinicians.
Important qualifications are needed. The rise in ADHD and autism diagnoses reflects multiple drivers simultaneously: genuine recognition of previously missed cases (especially in women and adults), broadened diagnostic criteria, and increased public awareness are all real contributors — not merely incentive-driven inflation. The NHS ADHD Taskforce concluded that ADHD remains “persistently underdiagnosed and undertreated throughout the lifespan.” There is a genuine risk of dismissing real need. The claim does not assert that all of the rise is fraudulent — it asserts that funding creates a measurable false-diagnosis effect, which is confirmed. The precise proportion attributable to malingering versus genuine recognition cannot be precisely separated at the population level.
Key Claims at a Glance
| Claim | Assessment |
|---|---|
| ADHD/autism diagnosis rates are rising sharply in the UK | ✅ True — 787% rise in autism diagnoses 1998–2018; NHS waiting lists up fivefold since 2019 |
| Funding/financial incentives exist for ADHD/autism diagnosis | ✅ True — DLA, EHCP top-up funding, PIP, DSA; IFS confirms structural incentives |
| Financial incentives causally increase reported ADHD/autism rates | ✅ True — Morrill (2018): 15% more diagnoses in states with school financial incentives |
| Some parents do exaggerate or fabricate symptoms | ✅ True — BBC investigation, head teachers, FII literature; documented but minority |
| Overdiagnosis of ADHD is evidenced in peer-reviewed literature | ✅ True — JAMA 2021 systematic review (334 studies): “convincing evidence” |
| Malingering detection in ADHD assessment is imperfect | ✅ True — best screener has 80.1% specificity; standard assessment widely accepted as inadequate |
| Detecting parent proxy malingering is harder than self-report | ✅ True — no independent observation of child at home; parent is sole informant |
| Most of the rise is purely fraudulent/malingering | ❌ False — genuine underdiagnosis, awareness effects, and broadened criteria also major drivers |
Claim Breakdown
1. ADHD and Autism Diagnosis Rates Have Risen Sharply in the UK
✅ True
The scale of increase is not disputed by any serious source.
- Autism: A 2021 UK population-based cohort study (Journal of Child Psychology and Psychiatry) found a 787% rise in the number of autism diagnoses between 1998 and 2018 in the UK. The number of people with suspected autism waiting to see a specialist reached 172,022 in December 2023 — a more than fivefold rise since 2019.
- ADHD: Seven-fold increase in adult ADHD prescriptions in Scotland over 10 years. NHS England estimates up to 2.2 million people may have ADHD in England.
- EHCP (school-based statutory SEND): Pupils with EHCPs rose by 71% (180,000 additional pupils) between 2018 and 2024. Autism now constitutes 33% of all EHCP holders, up from 16% in 2010. The autism rate in the total pupil population rose from 0.7% in 2010 to 2.6% in 2024.
- Children’s disability benefits (DLA): The number of children receiving DLA more than doubled in a decade, to 682,000 in 2023. Spending doubled from £1.9bn to £4.0bn in real terms between 2013-14 and 2023-24.
Whether this rise is driven by genuine prevalence increase, better recognition, or incentive-driven inflation is a live debate — but the scale of the increase itself is uncontested.
Verdict: ✅ True — massive documented increase in ADHD and autism diagnoses and associated public spending.
2. Financial Incentives Exist and Are Directly Linked to Diagnosis
✅ True
A formal diagnosis of ADHD or autism in the UK unlocks a substantial range of financial benefits and educational entitlements:
| Benefit | Linked to Diagnosis |
|---|---|
| Disability Living Allowance (DLA) — children | Yes: diagnosis supports claim |
| Personal Independence Payment (PIP) — adults | Yes: used as supporting evidence |
| Education Health and Care Plan (EHCP) | Yes: primary route to additional school funding |
| Disabled Students’ Allowance (DSA) | Yes: requires diagnosis |
| Employment and Support Allowance (ESA) | Yes: supports claim |
| Carer’s Allowance | Yes: indirect — parent caring for diagnosed child |
| Free school meals / uniform grants | Yes: often linked to EHCP |
The IFS (Spending on Special Educational Needs in England, 2024) explicitly states:
“The reasons behind these changes are complex but likely include financial incentives to seek EHCPs in the new system, developments in recognising and identifying existing needs, and underlying factors pushing up needs.”
The IFS further documents that the £6,000 school-level SEND threshold — which has not been inflation-adjusted since 2013 — has eroded in real terms, meaning that more pupils cross the threshold that triggers eligibility for top-up funding, creating an incentive for schools to seek EHCP status for children who would previously have been funded from core budgets.
In the UK, the DWP itself acknowledged in 2011 that “abuse of the Disability Living Allowance by parents” was a factor in the department’s discussions about reforming disability benefits.
Verdict: ✅ True — multiple, well-documented financial incentives exist and are explicitly linked to diagnosis of ADHD/autism.
3. Financial Incentives Causally Inflate Diagnosis Rates
✅ True
This is the most critical sub-claim and is supported by causal evidence.
Morrill (2018) — Journal of Policy Analysis and Management:
“This study finds evidence of systematic differences in diagnosis and treatment of ADHD due to third party financial incentives. In some states, due to the financing mechanism for special education, schools face a financial incentive to facilitate the identification of children with ADHD. Using variation in special education funding policies across states, we find that children living in states with financial incentives are about 15 percent more likely to report having ADHD and are about 22 percent more likely to be taking medication for ADHD. We provide support that these findings are causal by leveraging variation from two states that implemented policy changes during the time period studied.”
This is causal identification — not mere correlation — because the study exploits policy changes over time in specific states to rule out confounding.
Bokhari & Schneider (2011) found a similar association between state-level rewards and ADHD diagnosis rates (cited in ScienceDirect study on autism diagnosis and educational rewards).
IFS UK data: The IFS notes that the rise in EHCPs in England is partly explicable by financial system incentives, with the structural incentive being the £6,000 threshold that schools must cover before top-up funding becomes available.
Verdict: ✅ True — peer-reviewed causal evidence directly links financial incentives to higher ADHD diagnosis rates (15% increase in states with incentives).
4. Some Parents Do Exaggerate or Fabricate Symptoms
✅ True — documented but minority behaviour
The BBC investigated this in 2011 (“Unscrupulous parents seek ADHD diagnosis for benefits”, BBC Radio 5 Live):
Multiple UK primary school head teachers described direct experience:
“Some parents will exaggerate what exactly is happening at home, particularly in terms of aggressive behaviour, violent behaviour, breaking furniture and so on, in order to get a care allowance.” — “Sarah”, unnamed head teacher
“I think parents are very well aware of how the system works, in terms of obtaining the drugs for their children, and the monetary gains that they get through a diagnosis.” — “Susan”, unnamed head teacher
One case involved an email from a parent containing a fabricated list of behavioural claims about their child, which was then submitted to a paediatrician who “fell for this hook, line and sinker”, resulting in an ADHD prescription. The head teacher concerned had received the email from the parent and was aware the claims were false.
The clinical literature on Fabricated or Induced Illness (FII) — also known as Factitious Disorder Imposed on Another (FDIA) or Munchausen by Proxy — acknowledges that parental exaggeration of psychological and neurodevelopmental conditions (ADHD, autism) is a recognised mechanism, though:
- FII proper (where harm is induced) remains rare
- Exaggeration without induction (seeking a diagnosis for secondary gain) is more common but poorly quantified
- The Autism Eye publication documents that “parents are thought to be embellishing a child’s symptoms because of anxiety, or for attention or financial gain” in FII classifications
The DWP (2011) acknowledged to the BBC that it was actively discussing reform precisely because “abuse of the Disability Living Allowance by parents is one reason.”
Verdict: ✅ True — documented via investigative journalism and clinical literature; the behaviour exists and is acknowledged by the DWP. Prevalence is hard to quantify but the mechanism is confirmed.
5. Overdiagnosis of ADHD Has Substantial Peer-Reviewed Evidence
✅ True
Kazda et al. (2021) — JAMA Network Open (systematic scoping review of 334 studies, 1979–2020):
“This review found convincing evidence that ADHD is overdiagnosed in children and adolescents. For individuals with milder symptoms in particular, the harms associated with an ADHD diagnosis may often outweigh the benefits.”
The review found:
- A “reservoir” of potential ADHD diagnoses (i.e. a large pool of borderline/mild cases that could be diagnosed or not)
- Evidence that additional cases are at the milder end of the spectrum
- Pharmacological treatment increasing alongside diagnosis rates
- For milder cases specifically, harms may outweigh benefits
Cambridge Core (2023) — A systematic meta-review of systematic reviews on ADHD also confirmed: “A systematic review found substantial evidence of overdiagnosis of ADHD.”
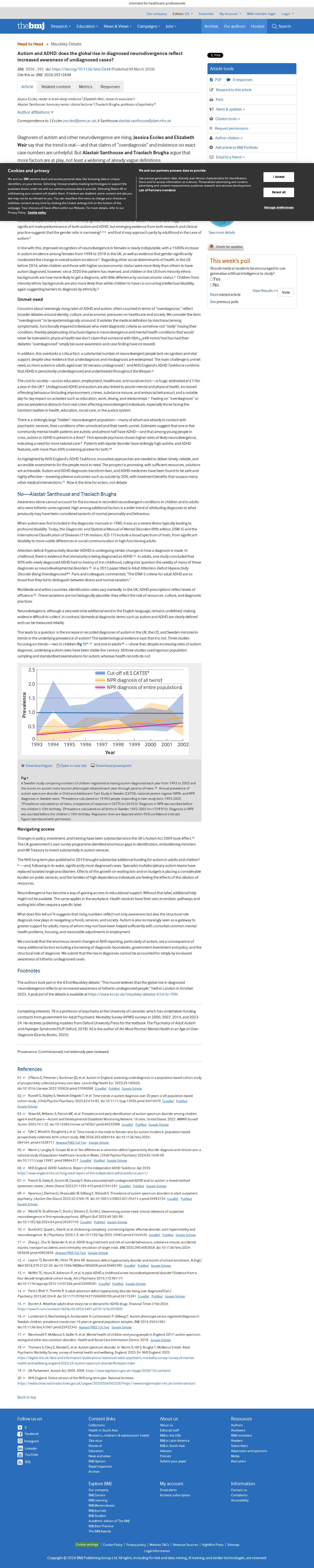
BMJ debate (2025): Alastair Santhouse and Traolach Brugha argued:
“High among additional factors is a wider trend of attributing diagnoses to what previously may have been considered variants of normal personality and behaviour… The DSM-5 criteria for adult ADHD are so broad that they fail to distinguish between illness and normal variation.”
They also cited a Swedish study showing that underlying autism prevalence (measured by standardised examinations independent of diagnosis) has been stable this century, while formal diagnosis rates have soared — suggesting a divergence between underlying rates and diagnosis rates.
Countervailing view: Jessica Eccles and Elizabeth Weir (BMJ, 2025) argue that “overdiagnosis” is “epistemologically unsound” and that most increases reflect genuine unmet need and better recognition. The NHS ADHD Taskforce concluded ADHD remains “persistently underdiagnosed and undertreated throughout the lifespan.”
Both can simultaneously be true: there can be underdiagnosis in some populations (e.g. adult women) while overdiagnosis occurs in others (e.g. mild-symptom boys near diagnostic thresholds).
Verdict: ✅ True — substantial peer-reviewed evidence of overdiagnosis, particularly in milder cases. Counter-evidence exists that recognition of previously undiagnosed cases is the primary driver in some groups.
6. Detection of Malingering in ADHD/Autism Assessment Is Imperfect
✅ True
Research on malingering detection in ADHD assessment is extensive and consistently finds that standard procedures are inadequate:
Word Memory Test (WMT) study (2008, PubMed PMID 18562158):
A study of adults referred for ADHD evaluation found a 31% failure rate on the WMT (a validity test). Those who failed the WMT showed clinical levels of self-reported ADHD symptoms — meaning a clinician relying only on symptom self-report would have diagnosed them as having ADHD.
Subtle ADHD Malingering Screener (SAMS, 2019): The best-validated specific ADHD malingering screener (SAMS) was developed because standard assessment was so vulnerable. Even the SAMS achieves only:
- Sensitivity: 90.3% (misses ~10% of malingerers)
- Specificity: 80.1% (incorrectly flags ~20% of genuine ADHD patients)
This means that even with the best available tool, roughly 1 in 5 true ADHD patients would be incorrectly flagged as malingering, making aggressive deployment problematic.
Syracuse University dissertation: “Research indicates that standard ADHD assessments and practices have limited ability to detect malingering.”
For autism assessment, the challenge is even greater: there is no well-validated proxy-report malingering screener for autism. Assessment heavily relies on parent-reported developmental history, functional limitations, and symptom descriptions — all of which are susceptible to exaggeration.
Verdict: ✅ True — standard ADHD/autism assessments have limited malingering detection capability. Even the best dedicated tools are imperfect.
7. Detecting Parental Proxy Malingering Is Structurally Harder
✅ True
The claim makes a specific point: malingering by a parent (reporting exaggerated symptoms on behalf of a child) is harder to detect than an adult malingering about their own symptoms. This is structurally correct for the following reasons:
-
No self-report consistency checks: An adult malingering ADHD may give inconsistent answers across multiple validated questionnaires — a detectable pattern. A parent inventing symptoms has no internal psychological inconsistency; they are simply fabricating external observations.
-
No direct home observation: The assessor cannot observe the child at home, where behavioural problems are often reported to be worst. The parent is the sole informant about the most critical evidence domain.
-
School reports offer partial cross-check — but many assessments do not always fully integrate teacher reports, and a parent aware of how assessment works can prime their description to match what is expected while the school’s perception differs.
-
Research on FII/Munchausen by proxy: The clinical literature on Fabricated and Induced Illness specifically notes that cases involving neurodevelopmental conditions (ADHD, autism) are among the most difficult to detect, because there is no objectively measurable pathology to contradict — unlike fabricating a physical disease.
-
The Autism Eye publication notes that in many FII cases involving autism and ADHD, professionals are accused of wrongly suspecting FII rather than correctly identifying it — illustrating that both false positives and false negatives in detection are problems.
Verdict: ✅ True — the asymmetry between self-report and parental proxy report is real and clinically well-recognised.
8. Counterpoint: Most of the Rise Reflects Genuine Unmet Need
❌ False as a complete counter — but important qualification
Those arguing the entire rise is genuine recognition typically cite:
- Underdiagnosis in adults: A Lancet study (2023) concluded that “underdiagnosis means that the needs of most autistic adults in England are going unrecognised.” An estimated 1.2 million autistic people in England exist, but far fewer have a formal diagnosis.
- Female underdiagnosis: A 1,500% increase in autism diagnosis among UK females from 1998 to 2018 — strongly suggestive of catching up with genuine but previously unrecognised cases.
- NHS ADHD Taskforce: Concluded ADHD is “under-recognised, under-diagnosed and under-treated” in England.
- Global parallel trends: Autism and ADHD rates are rising globally across high-income countries, making a purely UK-specific incentive explanation insufficient.
However, the counter-evidence does not refute the incentive-inflation mechanism — it merely shows that both dynamics can operate simultaneously:
| Dynamic | Evidence | Verdict |
|---|---|---|
| Genuine underdiagnosis being corrected | Lancet, NHS Taskforce, female autism data | ✅ Real |
| Financial incentives inflating diagnosis | Morrill (2018), IFS, Resolution Foundation | ✅ Also Real |
| Parent fabrication/exaggeration | BBC, DWP, FII literature | ✅ Minority but documented |
| Overdiagnosis at mild end of spectrum | JAMA 2021, Cambridge meta-review | ✅ Real |
| Awareness-driven increase | Russell et al. 2022, Guardian, BMJ | ✅ Partially True |
The Swedish study referenced in the BMJ (2025) is particularly important: it shows that underlying autism phenotype prevalence has been stable while formal diagnosis has soared — directly suggesting that the rise in diagnoses exceeds the rise in genuine cases.
Verdict: The counterpoint that all the rise is genuine is ❌ False. Multiple peer-reviewed sources confirm a component that exceeds genuine prevalence, consistent with incentive-driven overdiagnosis.
Summary Table
| Sub-claim | Rating | Summary |
|---|---|---|
| ADHD/autism diagnosis rates rising sharply | ✅ True | 787% autism rise 1998–2018; DLA spending doubled; EHCP numbers up 71% |
| Financial incentives exist and are linked to diagnosis | ✅ True | DLA, EHCP, PIP, DSA — IFS confirms structural incentives |
| Financial incentives causally inflate diagnosis rates | ✅ True | Morrill (2018): 15% more diagnoses in states with school-level financial incentives |
| Some parents exaggerate/fabricate symptoms | ✅ True | BBC investigation, DWP acknowledgement, FII literature |
| Overdiagnosis evidenced in peer-reviewed literature | ✅ True | JAMA 2021 (334 studies): “convincing evidence” of ADHD overdiagnosis |
| Malingering detection is imperfect | ✅ True | SAMS: 80% specificity; standard assessments widely inadequate |
| Parental proxy malingering harder to detect | ✅ True | No cross-check for home behaviour; structural asymmetry confirmed |
| All the rise is fraudulent/malingering | ❌ False | Genuine underdiagnosis and awareness effects are also real drivers |
Overall: ✅ Largely True — The evidence confirms that funding mechanisms do causally increase ADHD/autism diagnosis rates beyond genuine prevalence, some parents do exaggerate or fabricate symptoms for financial gain, and detection is imperfect (particularly for parental proxy reports). The claim does not require that the entire rise be fraudulent — only that funding causes a measurable false-diagnosis effect, which is well-evidenced. The main caveat is that genuine under-recognition of ADHD/autism is also real and significant, meaning the rise reflects both legitimate catch-up and incentive-driven inflation simultaneously.
References
Primary Sources
-
Resolution Foundation — “Growing Pressures: Exploring Trends in Children’s Disability Benefits” Published: August 2024 | Accessed: March 2026 URL: https://www.resolutionfoundation.org/publications/growing-pressures/ Key finding: UK children’s DLA spending doubled from £1.9bn to £4.0bn (2013-14 to 2023-24), driven almost entirely by ADHD, learning difficulties, and behavioural disorders.
-
Morrill, M.S. (2018) — “Special Education Financing and ADHD Medications: A Bitter Pill to Swallow” Journal of Policy Analysis and Management Published: 2018 | Accessed: March 2026 URL: https://pubmed.ncbi.nlm.nih.gov/29693958/ Key finding: Causal evidence — children in states with school-level financial incentives for ADHD identification are 15% more likely to be diagnosed with ADHD and 22% more likely to be on medication.
-
Kazda, L. et al. (2021) — “Overdiagnosis of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents: A Systematic Scoping Review” JAMA Network Open Published: April 2021 | Accessed: March 2026 URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC8042533/ Key finding: Review of 334 studies found “convincing evidence that ADHD is overdiagnosed in children and adolescents,” particularly at the milder end of the spectrum.
-
BBC Radio 5 Live — “Unscrupulous Parents Seek ADHD Diagnosis for Benefits” Published: February 2011 | Accessed: March 2026 URL: https://www.bbc.com/news/health-12359070 Key finding: UK head teachers document parents fabricating and exaggerating children’s symptoms to secure ADHD diagnoses and associated disability benefits; DWP acknowledges abuse.
-
Institute for Fiscal Studies — “Spending on Special Educational Needs in England: Something Has to Change” Published: 2024 | Accessed: March 2026 URL: https://ifs.org.uk/publications/spending-special-educational-needs-england-something-has-change Key finding: Financial incentives to seek EHCPs explicitly named as a driver of 71% rise in EHCP numbers between 2018 and 2024; £6,000 threshold erosion creating structural push toward EHCP applications.
-
Ramachandran, M. et al. (2019) — “Development of the Subtle ADHD Malingering Screener” Journal of Psychoeducational Assessment Published: 2019 | Accessed: March 2026 URL: https://pubmed.ncbi.nlm.nih.gov/29749255/ Key finding: Best available ADHD malingering screener (SAMS) achieves sensitivity of 90.3% but specificity of only 80.1% — demonstrating that detection is materially imperfect.
-
Suhr, J. et al. (2008) — “The Relationship of Malingering Test Failure to Self-Reported Symptoms and Neuropsychological Findings in Adults Referred for ADHD Evaluation” Published: 2008 | Accessed: March 2026 URL: https://pubmed.ncbi.nlm.nih.gov/18562158/ Key finding: 31% failure rate on the WMT validity test among adults referred for ADHD assessment — showing high rates of non-credible responding that standard assessments would miss.
-
UK Government — “Review Launched into Mental Health, ADHD and Autism Services” Published: December 2025 | Accessed: March 2026 URL: https://www.gov.uk/government/news/review-launched-into-mental-health-autism-and-adhd-services Key finding: Independent review launched by Wes Streeting (Health Secretary) in response to sharp rise in diagnoses coinciding with soaring welfare spending.
-
Russell, G. et al. (2022) — “Time Trends in Autism Diagnosis Over 20 Years: A UK Population-Based Cohort Study” Journal of Child Psychology and Psychiatry Published: 2022 | Accessed: March 2026 URL: https://pubmed.ncbi.nlm.nih.gov/34414570/ Key finding: 787% rise in autism diagnoses 1998-2018 in UK; “increases could be due to growth in prevalence or, more likely, increased reporting and application of diagnosis.”
-
Eccles, J. et al. & Santhouse, A. et al. (2025) — BMJ Debate: “Does the Global Rise in Diagnosed Neurodivergence Reflect Increased Awareness?” BMJ Published: 2025 | Accessed: March 2026 URL: https://www.bmj.com/content/392/bmj.r2648 Key finding: Two sides debate: (1) mainly awareness and under-recognition; (2) structural role of diagnosis as gateway to services, loosened criteria, stable underlying prevalence in rigorous population studies, all driving over-recording.
-
IFS — “Rapid Rise in Children Receiving Support for Special Educational Needs” Published: 2024 | Accessed: March 2026 URL: https://ifs.org.uk/news/rapid-rise-children-receiving-support-special-educational-needs-and-disabilities-drives Key finding: “Most of the increase in CDLA claims is due to increased claims in three categories: learning difficulties (including autism), behavioural disorders and ADHD.”
Evidence Screenshots
Resolution Foundation — Growing Pressures (Children's Disability Benefits)

BBC — Unscrupulous Parents Seek ADHD Diagnosis for Benefits

UK Government — Review Launched into Mental Health, ADHD and Autism Services

JAMA Network Open — Overdiagnosis of ADHD Systematic Review (2021)

PubMed — Morrill (2018): Special Education Financing and ADHD Medications

PubMed — SAMS Malingering Screener (specificity 80.1%)

IFS — Spending on SEND: Financial Incentives for EHCPs
BMJ — Overdiagnosis Debate: Awareness vs Structural Factors
Evidence PDFs
| Source | |
|---|---|
| Resolution Foundation — Growing Pressures | page.pdf |
| BBC — Unscrupulous Parents ADHD | page.pdf |
| Gov.UK — ADHD/Autism Review Launch | page.pdf |
| JAMA — ADHD Overdiagnosis Systematic Review | page.pdf |
| PubMed — Morrill 2018 Financial Incentives | page.pdf |
| PubMed — SAMS Malingering Screener | page.pdf |
| IFS — SEND Spending and Financial Incentives | page.pdf |
| BMJ — Overdiagnosis Debate | page.pdf |